
Transforming Struggling Rural Hospitals into Centers of Confidence
Over the last 30 years, urban health systems have implemented a rural affiliation strategy of channeling specialty acute care patients (e.g., major surgery, cerebrovascular, neonate, cancer) from primary rural facilities in a “hub and spoke” model. The hub and spoke model promised that rural hospitals would have shared services and outpatient specialty clinical support to reduce overhead costs and keep most outpatient and basic acute care local. Health systems would make it easier to transport critically-ill patients to specialty hospitals, while offering support of specialists in providing local diagnostic and outpatient care. A great trade-off in theory.
A miserable reality in practice. Unfortunately, specialist physicians resisted the required travel time to support rural outpatient clinics and the hub and spoke became a one-way channel to funnel most patient care past the local rural hospital to the specialist clinics on the urban campuses. In fact, studies have shown that nearly 50% of rural patients now bypass their local hospitals and drive 30+ miles further for routine specialty and urgent care. Rural hospitals have lost more than 50% of their volume and now only provide care for FQHC clinics, emergent care and acute care for those unable to travel or afford the care provided at the regional health system campus.
Yet, rural hospitals are the life blood of rural counties. The closure of a rural hospital can significantly harm a local economy by causing job losses, reducing local spending, decreasing property values, and deterring new businesses from settling in the community, ultimately leading to a decline in per capita income and potentially a population decrease as residents seek healthcare elsewhere – essentially acting as a major economic setback for rural areas that heavily rely on the hospital as a major employer and service provider.
Now, health systems can make good on their “hub and spoke” promise by transforming their rural hospitals into “Centers of Confidence,” where the local population has trust that they will receive the same high quality of care as at the regional hospital. This requires a commitment to develop a telemedicine connection to remote specialty physicians from their main campus. By providing remote consultation and guidance by the same specialists that they travel to see at the regional hospital, local hospitals can improve patient access, cost, service and satisfaction. Specialty physicians can guide treatment in rural outpatient clinics, emergency rooms, operating rooms, ICU beds, nursing homes and even home health by remotely supporting primary physicians, ER physicians, hospitalists, general surgeons, nurse practitioners, medical assistants and social workers.
A new Center of Confidence operating model can repatriate the 50% of patients that are bypassing the local hospital and provide a new outlet for regional hospitals to solve their inpatient capacity problems with transfers for local hospital recovery stays.
However, a Center of Confidence operating model requires more than a telehealth connection. In fact, basic “zoom” telehealth solutions have failed so provide the level of care required. The new operating model requires a telemedicine 2.0 collaborative care model that integrates new roles, team relationships, practices, workflow and systems to deliver remote specialty care with confidence, for both the patient and the physicians. This includes:
- New Roles – a clinician extender role of a local caregiver who is specifically trained to provide onsite support for remote specialists to provide assessment, diagnosis, treatment and education.
- New Relationships – remote care teams that work together collaboratively under the guidance of the remote physician in a “treat and train” practice that continues to build clinician extender capability and remote physician productivity.
- New Practices – new telemedicine best practices that optimize the scheduling, delivery and recovery of care delivered by local caregivers under remote physician guidance.
- New Workflow – this new remote telemedicine model is called Coactive Care. It is different from ambulatory and acute care delivery models and provides a new collaborative model that optimizes remote care access, service, productivity, costs and patient outcomes.
- New Systems – Coactive Care needs more than basic telehealth – it requires a telemedicine 2.0 platform that supports the real-time collaborative care experience necessary for remote specialists to guide local clinician extenders in their shared patient care.
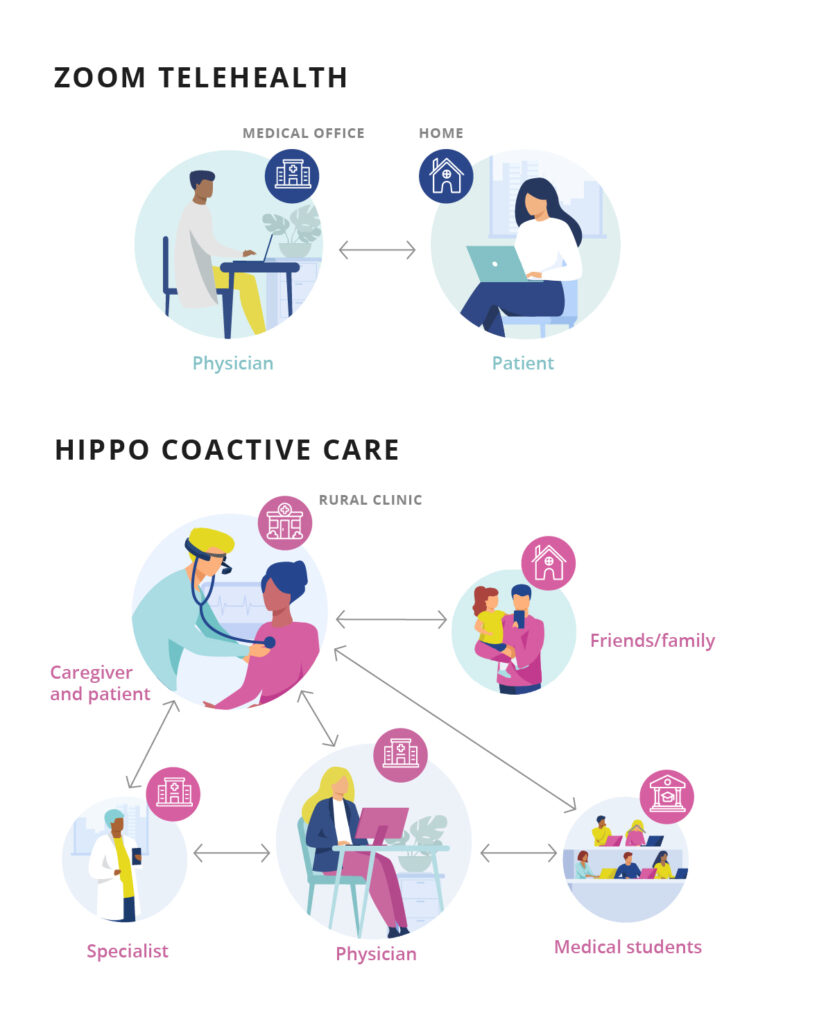
| ZOOM TELEHEALTH | HIPPO COACTIVE CARE |
|---|---|
|
One-on-one Primary Care
|
Multidisciplinary Specialty Care |
|
No additional participants |
Many participants: family, consults, med students, etc.
|
|
Physician does most of work |
Caregiver supports physician diagnosis |
|
Static TV view of patient |
“Eye of the clinician” view of patient & additional device views |
|
Didactic Interview care model |
Coactive care model, caregiver providing input |
|
Limited diagnostic input (RPM)
|
Nurse qualitative assessment, pictures and digital stethoscope
|
|
Generic Tele-meeting functions |
Purpose-built for complex Specialty Care
|
|
No local support for patient
|
Local Caregiver support and patient education
|
|
Physician requires key entry
|
Hands-free, voice-activated to focus on patient care
|
|
Basic diagnosis and treatment |
Advanced diagnosis and treatment |
|
Follow-up in Office if not better
|
Caregiver follow-up locally, with remote physician
|
Reviving rural hospitals into vibrant health Centers of Confidence for the community takes more than connection to the regional health EMR and telehealth systems. Centers of Confidence deliver the same regional specialist care to patients locally through an integrated Coactive Care team using clinician extenders, best practices, collaborative workflow and telemedicine 2.0 systems.